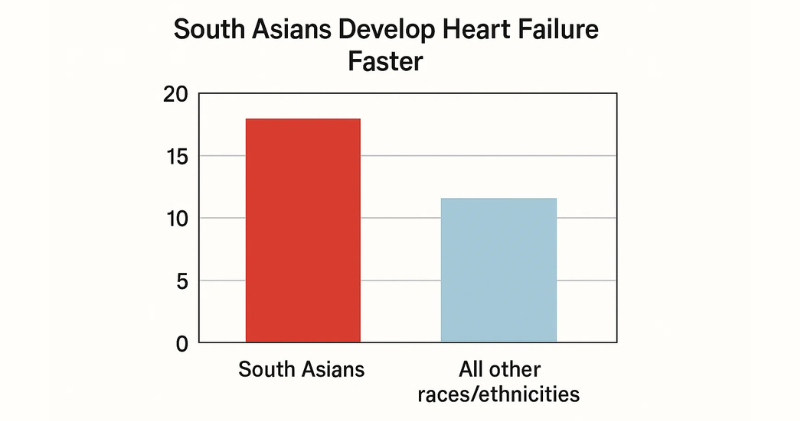
Did you know that South Asians develop heart failure 10-15 years earlier than other groups? While most people think heart problems happen to older adults, South Asians are getting heart failure in their 50s and 60s – sometimes even younger. This silent crisis is growing, but many families don’t know about it until it’s too late.
What Is Heart Failure, Really?
Heart failure doesn’t mean your heart stops working. It means your heart becomes too weak or too stiff to pump blood properly to the rest of your body.
Think of your heart like a water pump in your home. When the pump gets weak, water doesn’t flow well to all the rooms. Your body doesn’t get enough oxygen and nutrients, and fluid starts backing up in your lungs and legs.
Heart failure is NOT the same as a heart attack. A heart attack happens when blood flow to the heart is suddenly blocked. Heart failure develops slowly over months or years as the heart muscle gets weaker.
The scary truth: By the time most people notice symptoms, heart failure is already advanced. That’s why it’s called a “hidden” crisis.
Why South Asians Are More at Risk
Earlier Age of Onset
Studies from India show that South Asians develop heart failure at an average age of 56-61 years. In the United States, the average age is 72 years. That’s a 10-15 year difference.
Why does this happen? Several factors make South Asian hearts more vulnerable:
The Diabetes Connection
South Asians have 50% higher rates of diabetes than other groups. High blood sugar damages blood vessels and makes the heart work harder. Over time, this leads to diabetic cardiomyopathy – a type of heart muscle damage.
Even worse: Many South Asians have diabetes for years without knowing it. By the time it’s diagnosed, heart damage may have already started.
The “Thin Fat” Problem
South Asians can have dangerous belly fat even at “normal” weight. This visceral fat around organs releases harmful chemicals that:
- Increase inflammation
- Raise blood pressure
- Make insulin less effective
- Put extra strain on the heart
A person with BMI of 23 might look healthy but have the heart risk of someone much heavier.
Air Pollution Crisis
South Asian cities have some of the world’s worst air quality. 17 of the top 30 most polluted cities globally are in South Asia.
Air pollution causes:
- Increased inflammation in blood vessels
- Higher blood pressure
- More blood clots
- Heart muscle damage
Indoor pollution is also dangerous: 74% of South Asian households use wood, coal, or dung for cooking without proper ventilation.
Genetic Factors
Recent research shows South Asians have unique genetic risks:
MYBPC3 gene variant: 4-6% of South Asians (about 100 million people worldwide) carry a genetic variant that leads to heart muscle problems and eventual heart failure.
High Lipoprotein(a): South Asians naturally have higher levels of this “sticky” cholesterol that clogs arteries faster than regular cholesterol.
Cultural Risk Factors
- Tobacco use: Including bidis (cheap cigarettes) and smokeless tobacco
- Diet: Traditional foods high in refined carbs, saturated fats, and salt
- Low exercise: Studies show only 6.1% of South Asians exercise regularly vs. 21.6% of other groups
- Stress: Financial pressure, family obligations, and cultural expectations
Symptoms to Watch For (But Often Missed)
Heart failure symptoms develop slowly, so people often ignore them or blame aging. Watch for these warning signs:
5 Early Warning Signs of Heart Failure
- Unusual tiredness – feeling exhausted after normal activities
- Swelling – especially in feet, ankles, legs, or belly
- Shortness of breath – during activity or when lying flat
- Persistent cough – especially with white or pink foam
- Rapid weight gain – 2-3 pounds in a day or 5 pounds in a week
Women and elderly South Asians often have subtle symptoms:
- Feeling “just tired all the time”
- Trouble sleeping flat
- Less appetite
- Confusion or memory problems
Don’t ignore these signs. Many South Asians delay seeing doctors due to cost, cultural barriers, or thinking symptoms are “normal aging.”
The Diagnosis Problem
Shocking fact: Less than half of South Asians with high blood pressure have been diagnosed or treated. Many with heart failure aren’t getting proper care.
Why diagnosis is delayed:
- Symptoms blamed on aging or stress
- Limited access to healthcare in rural areas
- Cost of tests and medications
- Cultural belief that “fate” determines health
- Lack of awareness about heart failure
In developed countries: Even South Asian immigrants are underdiagnosed. They’re often not included in heart failure research studies, so doctors may not recognize their unique risk patterns.
What You Can Do Right Now
Good news: Heart failure can often be prevented or delayed with early action. Here’s your action plan:
Know Your Numbers
Ask your doctor to check:
- Blood pressure – should be under 130/80
- Blood sugar (HbA1c) – should be under 7% if you have diabetes
- Cholesterol panel – including ApoB and Lp(a) tests
- BMI and waist size – waist should be under 35 inches for women, 40 inches for men
Start Moving Daily
- Walk 30 minutes daily – this is the best medicine for your heart
- Take stairs instead of elevators
- Park farther away from stores
- Dance to Bollywood music at home
- Join community walking groups
Improve Your Diet Gradually
Add more:
- Vegetables and fruits (aim for 5 servings daily)
- Whole grains (brown rice, whole wheat)
- Fish, beans, and lentils
- Nuts and seeds
Reduce:
- Fried foods and ghee
- White rice and refined flour
- Sugary drinks and sweets
- Processed and packaged foods
- Salt (use herbs and spices instead)
Manage Stress
- Practice deep breathing or meditation
- Connect with family and friends
- Set realistic expectations
- Consider counseling if stress feels overwhelming
Get Regular Check-ups
- See your doctor every 6 months if you have diabetes or high blood pressure
- Don’t skip appointments due to cost – many community health centers offer affordable care
- Bring a family member to appointments to help remember instructions
Know Your Family History
- Ask relatives about heart disease, diabetes, and sudden deaths
- Share this information with your doctor
- Start screening earlier if you have strong family history
Moving Forward With Hope
Heart failure in South Asians is a serious problem, but it’s not hopeless.
The encouraging news:
- We now understand why South Asians are at higher risk
- New medications like SGLT2 inhibitors (Jardiance) can help prevent heart failure
- Early detection and treatment can add years to your life
- Simple lifestyle changes make a big difference
Remember:
- Heart failure often develops silently over years
- South Asians need to start prevention earlier than other groups
- Small changes today can prevent big problems tomorrow
- Knowledge is your most powerful tool
Don’t wait for symptoms. If you’re South Asian and over 35, especially with diabetes or high blood pressure, talk to your doctor about heart failure prevention. Your heart – and your family – will thank you.
The goal isn’t to live in fear, but to live with awareness. Every step you take toward better heart health is a step toward a longer, healthier life with the people you love.
Want to learn more? Read about “Heart Tests Every South Asian Should Ask For” and “Early Warning Signs Your Doctor Might Miss”
Citations:
Primary Study: Srinivasan N, Gullapalli N, Shah KS. “Highlighting the South Asian Heart Failure Epidemic.” Cardiac Failure Review, 2024; 10:e07. https://doi.org/10.15420/cfr.2023.21
Supporting Research:
- Trivandrum Heart Failure Registry (THFR) – showing mean age of heart failure onset at 61 years in Indians vs 72 years in US populations
- INTER-CHF study – demonstrating mean age of 56 years for heart failure presentation in Indians
- MASALA study (Mediators of Atherosclerosis in South Asians Living in America) – showing increased visceral fat and metabolic abnormalities
- PURE study – revealing low awareness and treatment rates for hypertension in South Asian countries (only 40% aware, 32% treated, 13% controlled)
- INTERHEART study – demonstrating low physical activity rates (6.1% vs 21.6%) and elevated Lp(a) as risk factors in South Asians
Always consult with your healthcare provider before making changes to your medical care or treatment plan.



