
Why do Heart Problems Show up so Early in South Asian Families?
Many South Asians have seen this happen.
A family member has a heart attack in their 40s. Someone develops heart failure in their early 50s. Often, this happens without much warning.
What makes it more confusing is that many people looked “healthy.” Their weight was not very high. Their cholesterol report did not seem alarming. Yet heart disease still appeared.
Doctors and scientists have been trying to understand this pattern for years. New research is now offering a clue. It points to a new type of heart disease linked not to blocked arteries, but to how the heart uses fat for energy. While studying this condition, researchers also looked at a natural substance called tricaprin to better understand what goes wrong inside the heart.
A Different Way Heart Disease can Begin
Most people think heart disease starts when arteries get blocked. That does happen, but it is not the only way the heart can fail. In this newly identified condition, the problem starts inside the heart cells themselves.
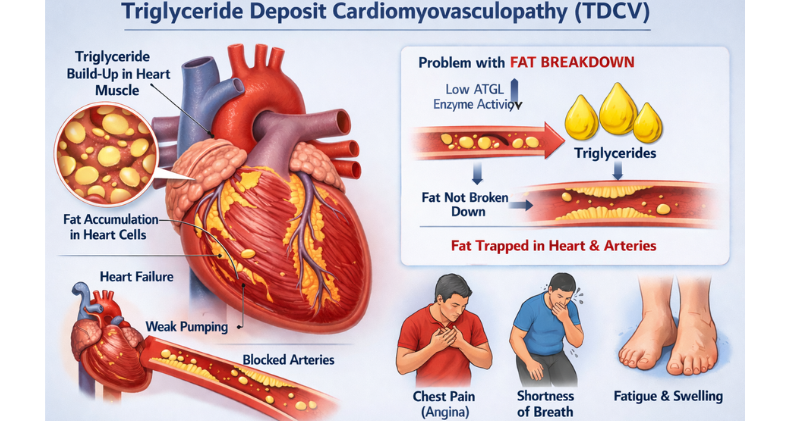
The condition is called Triglyceride Deposit Cardiomyovasculopathy (TDCV).
TDCV is a rare disease where triglycerides—a type of fat in the blood—build up inside heart cells.
The surprising part is this:
The heart has plenty of fat, but it cannot use it for energy. The heart needs energy every second to keep pumping. When it cannot access that energy, the heart muscle slowly becomes weak. Over time, this can lead to heart failure, chest pain, or poor blood flow.
Why This Matters for South Asians
This research matters because South Asians often have a different heart risk pattern than many other groups.
Studies show that South Asians:
Develop heart disease at a younger age
Often have higher triglycerides
Store more fat deep inside the body, around organs
Can have heart disease even when cholesterol looks “okay”
Because of this, doctors are learning that fat metabolism—how the body uses fat—may be especially important for South Asian heart health.
Some experts believe conditions like TDCV may be missed or underdiagnosed in Asian populations. This makes awareness important, even though the disease itself is rare.
Where Does Tricaprin come in?
While studying TDCV, researchers wanted to understand why heart cells could not use fat properly. This led them to study tricaprin.
Tricaprin is a natural fat. It breaks down into medium-chain fatty acids, which are easier for cells to use for energy.
Most fats need several steps and enzymes before the body can use them. Medium-chain fats are different. They can be used more quickly and with fewer steps. Because of this, scientists wondered if tricaprin could help heart cells that struggle to use stored fat.
It is important to understand that tricaprin is not a cure. It is being studied as a way to understand how energy problems inside the heart might be improved in very specific cases.
What Researchers Observed
Researchers in Japan studied people diagnosed with TDCV. Some patients were given tricaprin as part of their medical care. Others were not.
Over time, doctors noticed that patients who received tricaprin showed signs of better heart energy use. In some cases, heart function improved. Survival rates were also higher in the group that received tricaprin.
These findings were published in the European Heart Journal, a well-respected medical journal. However, the researchers were careful in their conclusions. The study involved a small number of patients and focused only on a rare disease.
This research helps scientists understand how heart cells fail—but it does not change everyday heart treatment yet.
What this Research does NOT Mean
Because the word “natural” is involved, it is easy for misunderstandings to spread. Let’s be clear.
This research does not mean:
Coconut oil treats heart disease
Everyone should take tricaprin
Supplements replace medical care
This study does not apply to most people with common heart disease. It is not a recommendation for self-treatment. It is part of ongoing scientific research.
What South Asian Families can Learn from This
Even though TDCV is rare, the message behind this research is important.
It reminds us that heart disease is not always about cholesterol alone. For South Asians, triglycerides, insulin resistance, and how the body uses fat may play a larger role than many people realize.
Simple steps still matter most:
Ask your doctor about triglycerides, not just total cholesterol
Learn your family heart history
Reduce sugar and refined carbohydrates
Stay physically active, even with daily walking
Get checked earlier, not later
Early awareness leads to early action.
A Hopeful Message
This research is not about fear. It is about understanding.
As scientists learn more about how the heart uses energy, they can develop better tests and better treatments in the future. For South Asians, this research highlights an important truth: heart disease risk can be hidden, but it is not unavoidable.
Knowledge helps families ask better questions and protect their hearts sooner.
Want to go Deeper?
Learn More: Heart Tests Every South Asian Should Know
Sources & Medical References
Hirano K et al.
Tricaprin improves cardiac function and survival in patients with triglyceride deposit cardiomyovasculopathy
European Heart Journal, 2023
https://academic.oup.com/eurheartj/article/44/15/1376/7039871Medical News Today
Natural supplement tricaprin may help people with new type of heart disease
https://www.medicalnewstoday.com/articles/natural-supplement-tricaprin-may-help-people-new-type-heart-diseaseWorld Health Organization
Cardiovascular Diseases (CVDs)
https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)Joshi P et al.
Risk factors for early myocardial infarction in South Asians
Journal of the American Medical Association (JAMA), 2007
https://pubmed.ncbi.nlm.nih.gov/17565082



